
( Paediatric Multi-inflammatory Syndrome temporally associated with SARS-CoV-2 )




THERE IS CURRENTLY NO OFFICIAL PUBLIC DATA AVAILABLE ON PIMS-TS IN THE UK
PIMS-TS was first publicly identified in April 2020. In the UK, we are aware of two systems of collecting PIMS data, to the best of our knowledge the following is correct.
The first system was initiated and carried out by Public Health England, now UKHSA, using the orange card system and collecting data at paediatrician level. Paediatricians were contacted monthly by UKHSA to report cases of PIMS-TS, Kawasaki Disease and Toxic Shock Syndrome. Reporting was carried out electronically and included a detailed clinical questionnaire. This data was then passed to the British Paediatric Surveillance Unit (BPSU) who are part of the Royal College of Paediatrics and Child Health (RCPCH) The BPSU then studied and analysed the data and have so far publish the first part of their study which covered the period March-June 2020. What we don’t know is whether the UKHSA also received this data and if so, how is it using it. Link to the BPSU study
But not all cases of PIMS-TS will reach paediatrician level and therefore not all cases will be included. There is also the worry that some children might present with atypical or incomplete PIMS-TS, as can be the case with Kawasaki disease, and might not seek medical advice or progress only to GP level. Also, as we know from group testimony, diagnosis is challenging, and misdiagnosis is common, so not all cases will be confirmed or recorded as PIMS-TS. Lastly, given that we are in a pandemic and the NHS is under immense pressure, we can’t be sure that PIMS-TS case submissions will be consistent.
Not all PIMS-TS cases will show a positive COVID-19 test result, so cases will not be recorded as COVID-19 admissions, even though PIMS-TS is a direct consequence of COVID-19 infection.
We are glad that data on PIMS-TS is being collected. But the only reason we know that it is, is through actively searching, asking questions and lots of emailing.
OPINION
In the UK there has been a continuing narrative of playing down the risks of COVID-19 to children. How many times have we heard...
- Children do not get ill with COVID-19
- PIMS-TS is a rare condition
- Children are not vectors of transmission of COVID-19?
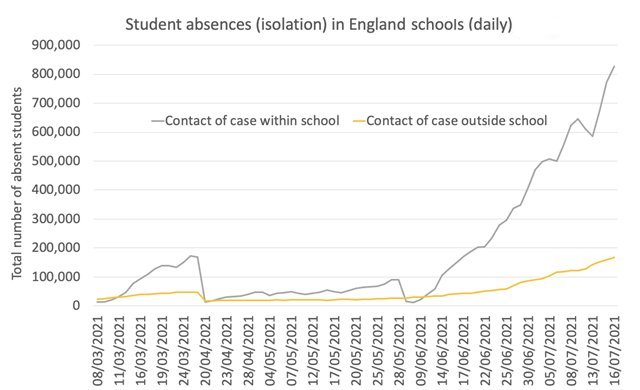
- Schools are safe
If those in positions of power, who these quotes come from, believe this to be true, why not release the data to support these claims? The graph below suggests otherwise...
PIMS-TS numbers have been occasionally mentioned in quotes in national newspapers. Here is a timeline on what we know.
78 cases - RCPCH Lancet paper April 1-May 10, 2020, based on PICU data.
268 cases - BPSU study part 1 March-June 2020, based on data from Paediatric level.
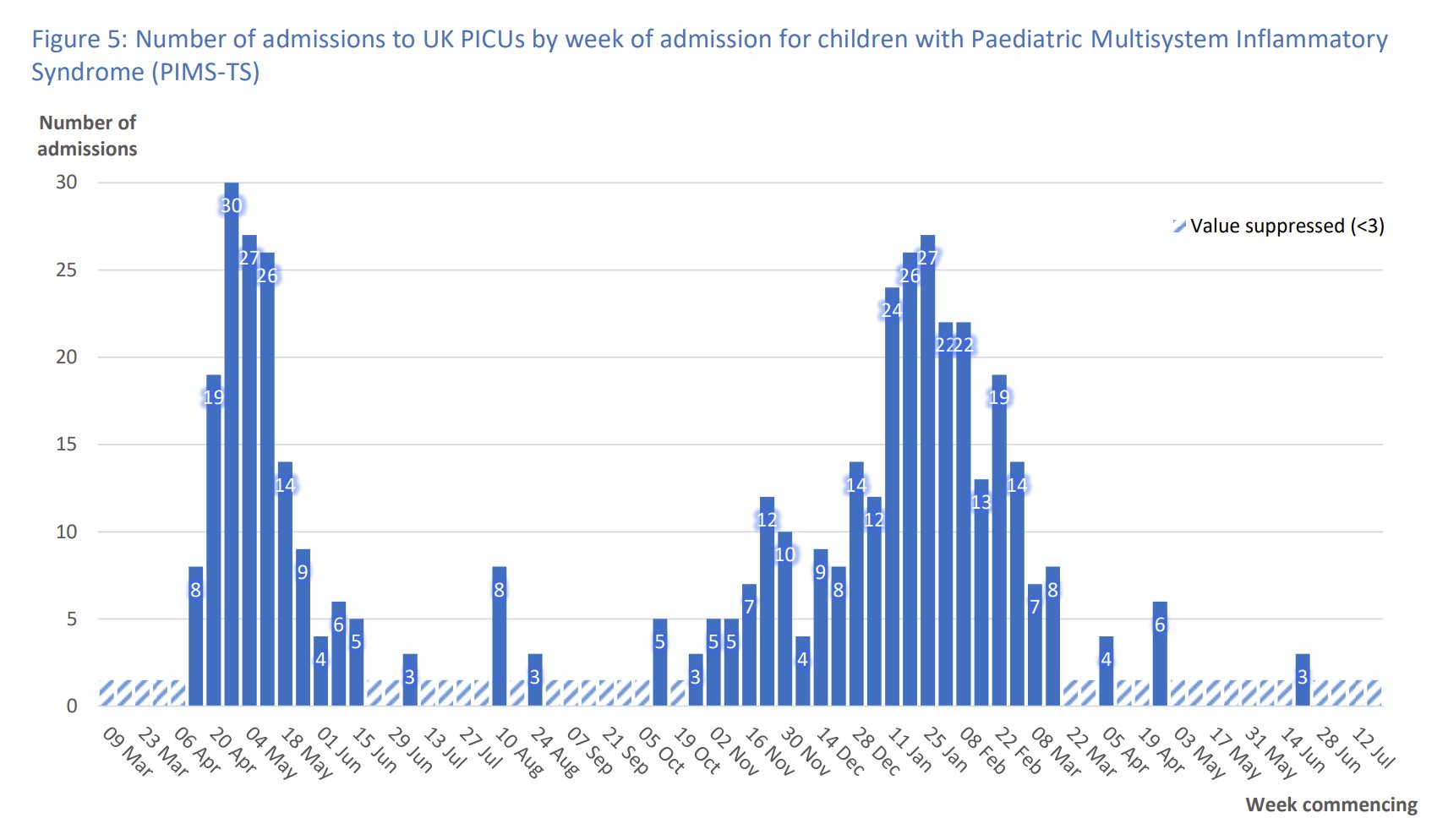
444 cases - in their annual report PICANet reported admissions into PICUs from March 2020-July 2021.
690 cases - BBC online article in February 2021 with quote by Dr Elizabeth Whittaker of RCPCH on PIMS cases admitted for emergency hospital treatment May 2020-Feb 21.
712 cases - in a Medrxiv article dated February 2021, whose contributors included Professor Russell Viner and Dr Elizabeth Whittaker.
2,593 cases + 2,270 KD cases - from NHS data sheet below, given in response to our FOI request, covering April 2020-February 2023. See notes below.
Our unofficial estimate of cases to April 2022: 2,500-3,000
Factors we have considered - were all cases included in the NHS data sheet - ie. was tertiary care included? Were atypical or incomplete cases of PIMS either not diagnosed or not included in the data? Have some of the cases of KD from the NHS data sheet in fact been PIMS cases? In our estimate, we have also made provision for cases declining since November 2021 due to the high number of children that have already been infected with COVID.
N.B. PICU COVID-19 and PIMS cases were analysed as one group from January-December 2020; thereafter they are recorded separately.
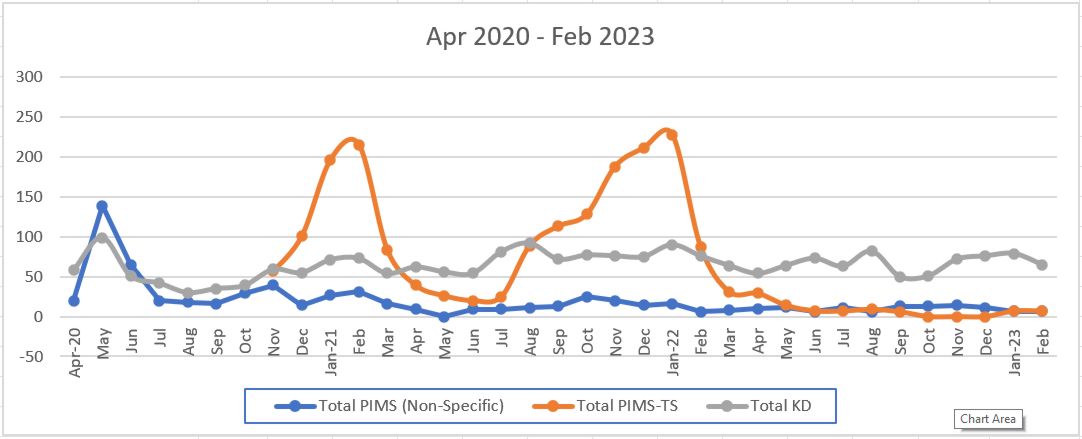
The table below illustrates the change in activity from R65 and M303 after the introduction of the U075 PIMS-TS COVID associated ICD10 code in November 2020. Please note that the data below is grouped by admission date and the introduction of U075 in November 2020 allowed any patient discharged after the introduction regardless of when admitted to have this code applied to their record where appropriate.
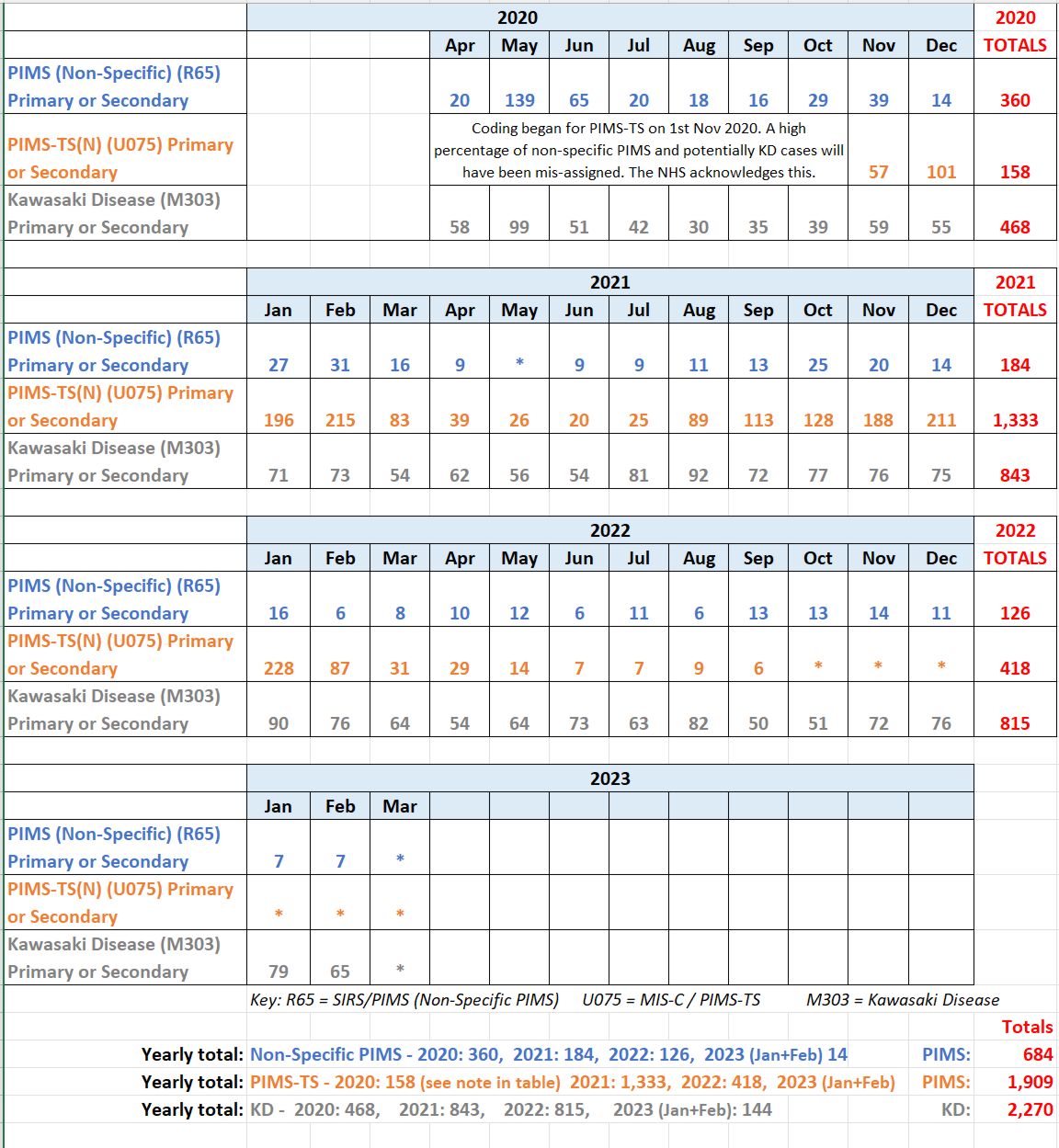
Before April 2020, PIMS was being observed but had not yet been defined and therefore not counted. The information gives more detail than previously but does raise some questions:
- Does this data relating to primary and secondary care omit any cases?
- Why are KD cases so high when they have substantially reduced in other parts of the world during the COVID-19 pandemic?
- Why are KD cases particularly high in the summer months, which is not typical?
- Could some of the KD cases in fact be PIMS?
We have asked NHS England for clarification on these points and how this data can be shared through the NHS websites.
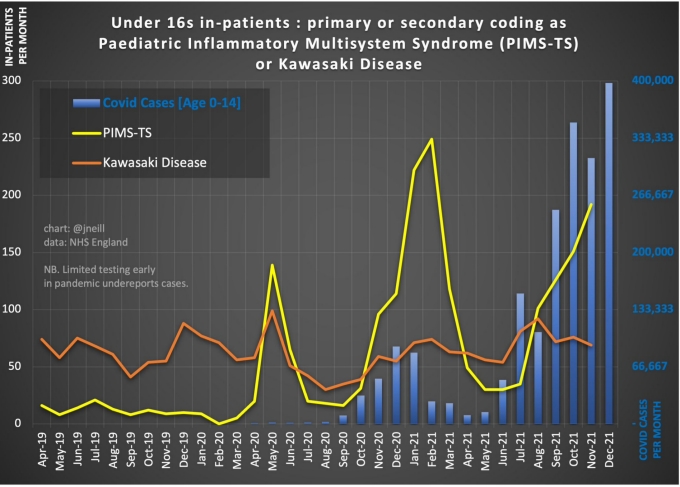
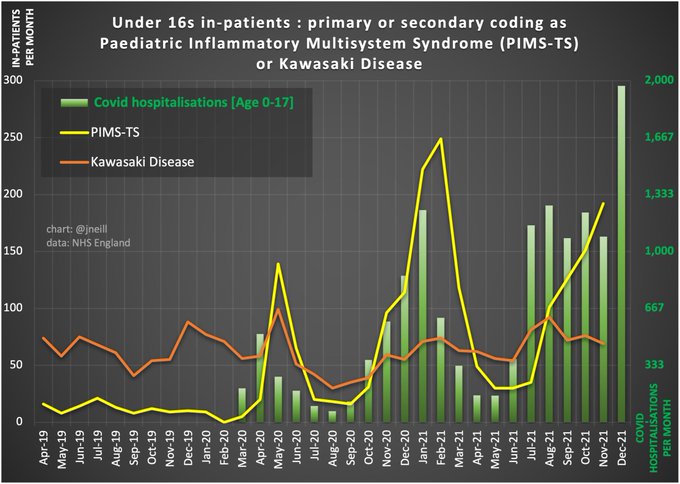
- In May 2020 some PIMS cases may have been classified as KD, as the syndrome was only just becoming evident.
- The peak in 2021 of PIMS cases/hospitalisations was played down.
- The upward trend of PIMS cases from July 2021 is lower as a percentage of COVID cases, perhaps due to many children having already had COVID followed by PIMS.
- As the data only goes to November 2021, how much has the recent Omicron wave affected PIMS cases?
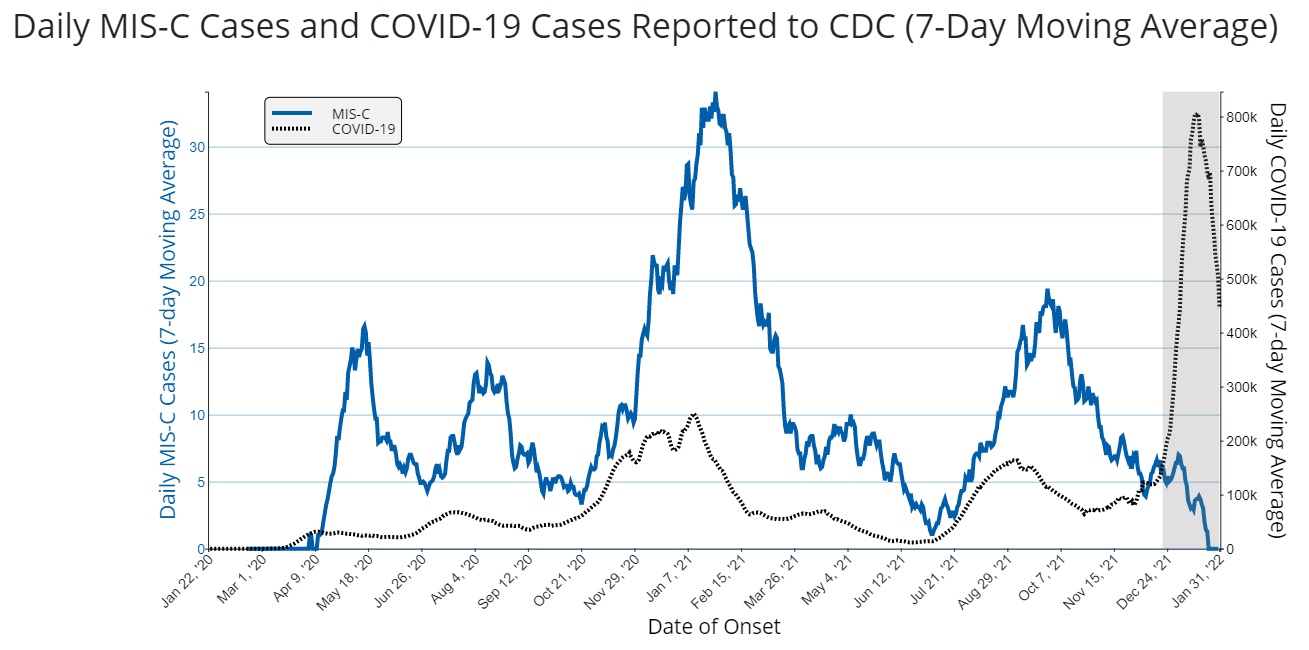
https://www.cdc.gov/mis/index.html
This graph from the CDC site seems to show a drop-off of MIS-C cases despite the Omicron wave, although the grey section on the right contains incomplete data.
For further analysis, follow this link.
Covid19-WHO
Data is beginning to be published from other countries, and we will add it as we become aware of it. Data from Germany 2022 (Use Chrome/Google translate if required as we think the page is only available in German at the moment.)
So why is data important?
For groups such as ours, who are trying to raise awareness of PIMS-TS, data and data analysis would help us in the following ways:
- To be aware of COVID/PIMS correlations and be able to predict when a spike might occur and target awareness in a timely manner
- To gauge the scale of aftercare required for our PIMS children and start to campaign for this.
- To look at the impact of vaccination on PIMS-TS cases in order to evaluate risk v benefit to inform national and individual decision making.
Death from PIMS-TS has only been entered on the ONS data from January 2022. It is entered under the name MIS-C as it is the WHO that is involved with its inclusion. So far there is 1 death recorded: follow this link to view/download the December 2021 excel file.
However, 3 deaths occurred before January 2022 and are recorded in this document.
This is important. As the scientists confirm, PIMS-TS is technically “rare”. The classification of a “rare” disease is less than 1 case in 2,000 of the general population. So, risk of getting PIMS-TS is low. But risk of becoming very ill with it is high. In many cases children suffer from medium to long term effects, and in some cases children suffer life changing damage.
"36% of patients in this study were found to have coronary artery abnormalities on echocardiography during PICU admission... although the long-term outcomes for these are unclear." The Lancet - Intensive Care admission Study
Without data on morbidity, long term after care and support (such as that being sought by Long Covid Kids) can’t be funded and organised. We have wealth of data on medium and long term after-effects of PIMS-TS that we are happy to share in order to ensure a robust system of follow-up and after-care for PIMS children.
Further Reading
Risk Factors for PICU admission and death with COVID and PIMS



