Brief synopsis of study
Around 90% of paediatricians took part in the study
Cases included fell within the RCPCH case definition of PIMS-TS and included children > 16 years
449 cases were reported, but after removing duplicates and those that didn’t fall into the definition or time frame, 343 remained :268 PIMS-TS, 13 with KD only, 2 with TTS and 4 with KD/TSS plus 56 that did not fully fit into any of these criteria.
Ethnicity, age and sex were compared for the 3 conditions
Presenting symptoms and laboratory findings were compared for the 3 conditions
Interestingly, 71.1% had a healthcare or non-healthcare keyworker parent
68.1% of cases were reported as PIMS-TS, with the remaining cases PIMS-TS plus TTS or KD
Cases in London were more likely in black children and the children were slightly older
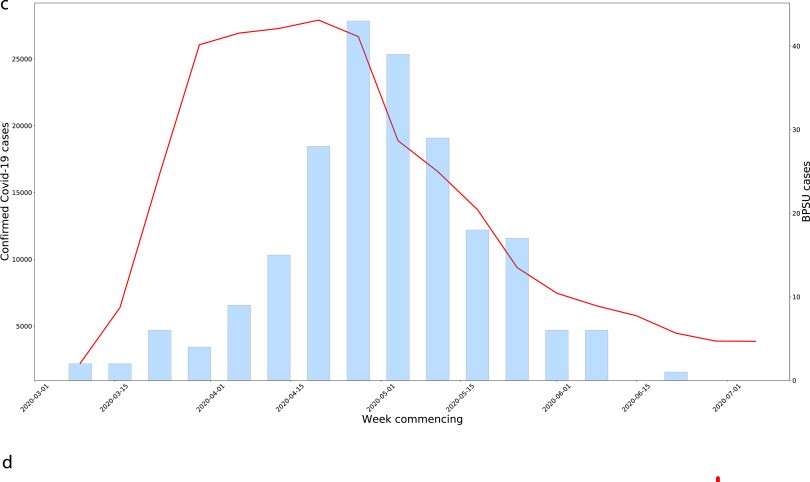
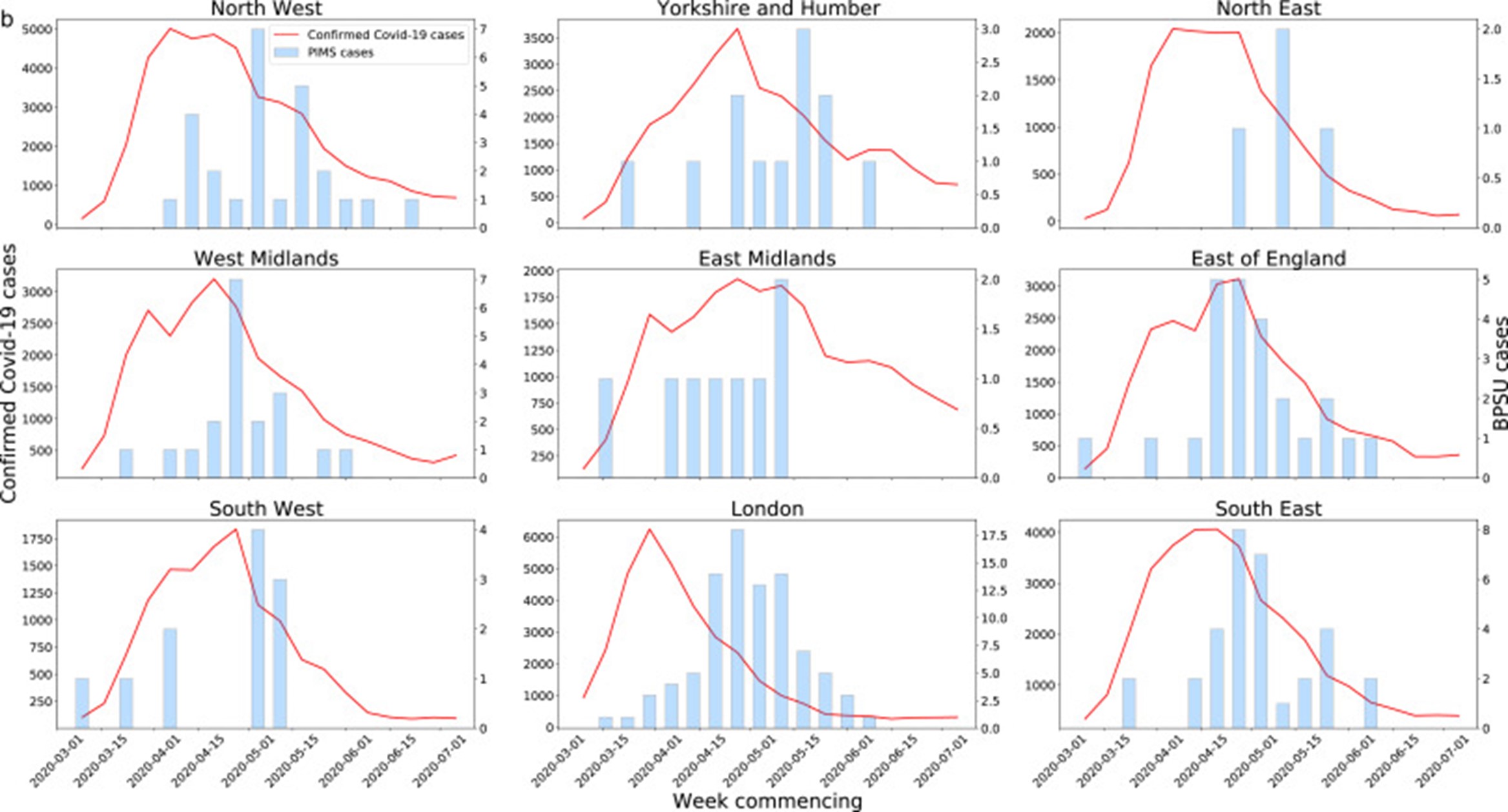
The median lag time between the COVID and PIMS-TS curve was 16.3 days
Only 44% of admissions included in this study were given a COVID test and this could have led to a misdiagnosis of PIMS-TS, possibly to KD or TSS.
14% of PIMS-TS cases were COVID positive and 63% had COVID antibodies.
Around 90% of paediatricians took part in the study
Cases included fell within the RCPCH case definition of PIMS-TS and included children > 16 years
449 cases were reported, but after removing duplicates and those that didn’t fall into the definition or time frame, 343 remained :268 PIMS-TS, 13 with KD only, 2 with TTS and 4 with KD/TSS plus 56 that did not fully fit into any of these criteria.
Ethnicity, age and sex were compared for the 3 conditions
Presenting symptoms and laboratory findings were compared for the 3 conditions
Interestingly, 71.1% had a healthcare or non-healthcare keyworker parent
68.1% of cases were reported as PIMS-TS, with the remaining cases PIMS-TS plus TTS or KD
Cases in London were more likely in black children and the children were slightly older
The median lag time between the COVID and PIMS-TS curve was 16.3 days
Only 44% of admissions included in this study were given a COVID test and this could have led to a misdiagnosis of PIMS-TS, possibly to KD or TSS.
14% of PIMS-TS cases were COVID positive and 63% had COVID antibodies.
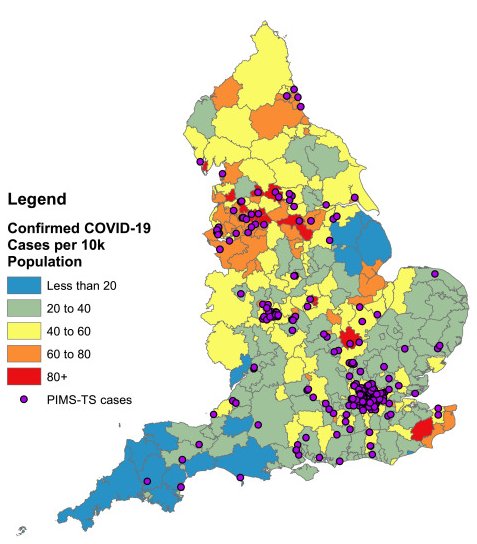
A map of all BPSU reports of PIMS-TS cases in England with postcode information (n = 246), alongside the rate of COVID-19 cases in LTLAs in England up to the 1st of July 2020